 Southwest Florida's Health and Wellness Magazine Health and Wellness Articles
Southwest Florida's Health and Wellness Magazine Health and Wellness Articles

By Robert Pollack, MD
In a recent article in the Wall Street Journal, it was noted that psychologists and psychiatrists are bracing for rising rates of Post-traumatic Stress Disorder (PTSD). PTSD is defined as a disorder that occurs after a person was exposed to death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence. The symptoms range from intrusive thoughts, avoidance behaviors, negative changes in cognition and mood, and a state of hyperarousal and decrease function. Treatments have ranged from cognitive focus to the use of pharmacotherapy. We now have some new developments in the treatment that we will address below.
PTSD has been with us for many years, and its treatment parallels the advances in medical science. When PTSD was treated in the mid-1970s, the primary focus was the use of group therapies and anti-depressant and anti-anxiety medications. Successes were minimal and the suffering was great. Fortunately, with better understanding of the neurobiology along with better science, we now have newer modalities that can help quiet the pain of PTSD symprtoms.
In a recent conference, an fMRI (Functional MRI) was taken and demonstrated several areas of the brain involved in PTSD. These would be the Anterior Cingulate Gyrus and the Amygdala (see photo). The Amydala is enlarged when faced with external stressors. The upper two spots are the Cingulate Gyri that are decreased in size in the presence of depression. For those suffering from PTSD, the Amygdala is highly activated and the Cingulate Gyrus and the Locus Ceruleus are dampened.
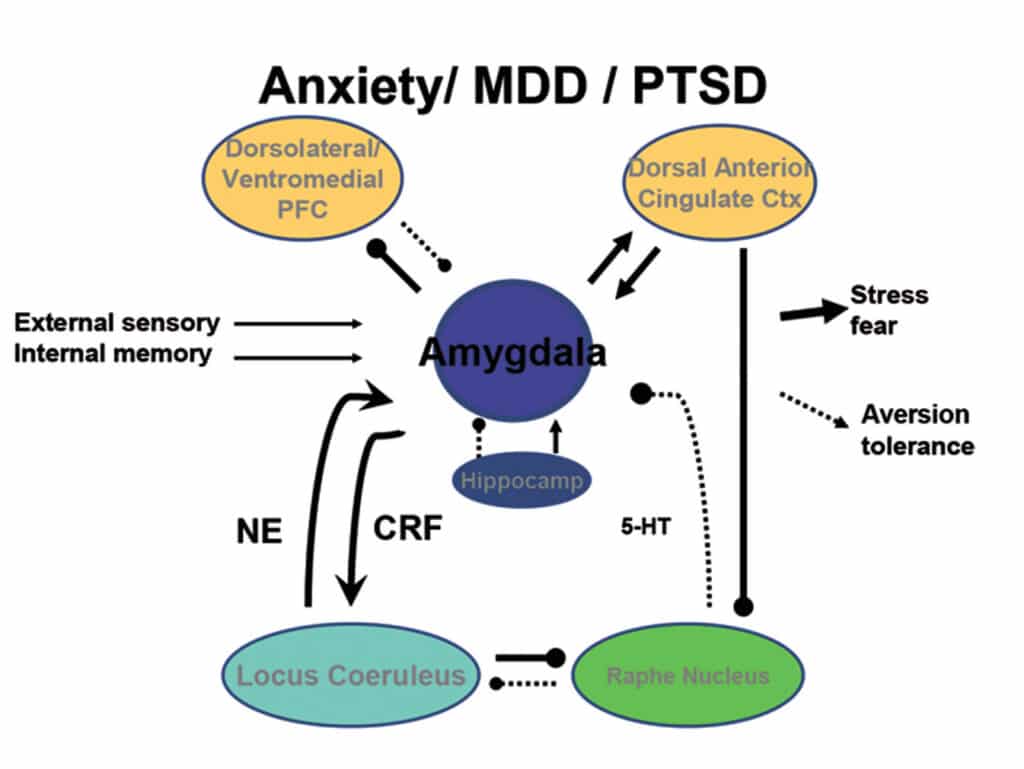
In the second picture we can see the relationship between the Amygdala and the areas that control mood (Cingulate area and the parts of the Prefrontal Cortex called Dorsolateral and Ventromedial). The Amygdala is the area that experiences the emotional trauma and then calls the other parts of the brain to generate different responses. These relationships set the stage for a non-medication, effective intervention.
In 1985 Dr. Mark George at the Medical University of South Carolina began his work and developed the use of electromagnetic stimuli to treat mood disorders. In doing this he was able to locate specific tracts in the brain and developed a technique referred to as Transcranial Magnetic Stimulation, TMS. This involved the application of stimuli over the dorsolateral prefrontal cortex. When placed on the left side, the depression is ameliorated and on the right side, the anxiety is abated. As of now this application takes 19 minutes and is repeated over 42 sessions (36 treatments and 6 tapering-off sessions) for depression and less for anxiety. This treatment has been successful for both depression and anxiety as well as PTSD.
Over the ensuing years Theta Burst Stimulation, TBS, was developed and added. It uses a 50Hz coil, instead of the 10 HZ coil, and treatments take 6 minutes 24 seconds over a period of 10 treatments. Results are comparable to the 10 Hz TMS treatments.
In the 1970s an anesthetic agent was developed named Ketamine. In addition to decreasing pain perception and levels of arousal, Ketamine seemed to have a mild dissociative property which made it an ideal tool for working with people suffering from PTSD. The mechanism revealed impact on BDNF levels which improves the ability to respond to therapy as well as decrease the degree of depression. Concomitantly, the Cingulate Gyrus, Hippocampus and Amygdala also respond to the medication. Treatment is often done by Infusion for 42 minutes in a setting which is carefully monitored. There are usually 6 sessions over a 2-week period. Conceptually, the infusion causes a brief dissociation (separation) between the horrific memories and the associated depression and anxiety. This allows for more effective types of talk therapy.
We have learned that the above treatments, when combined with different types of talk therapy, can be very successful. In some cases, combinations of the above treatments are used. This has increased the success rates for the patient. Additionally, once treatments are complete, patients can be monitored at home using the ITS Biometric System which allows patients to use their cell phones to track their Blood Pressure, Pulse, Respirations, PO2 levels, as well as PHQ9 (for depression), GAD7 (for anxiety) and the Rothman Index (a monitor of medical wellness). This process also keeps the patient in touch with his/her providers after the in-office treatments have decreased or stopped.
PTSD remains a multimodal illness that affects mood, anxiety and the ability to deal with life stressors. Many successful programs exist. What we have reviewed above reflects the advances in technologies that have added to the successful treatment of PTSD.
PASWFL.COM
6804 Porto Fino Cir #1, Fort Myers, FL 33912
Office: 239-332-4700
